The above comes from Michael Moore’s Sicko. Cuba’s healthcare system is a common talking point among those of Moore’s persuasion. However, a recent study should give us pause regarding some of the overly positive claims about Cuba’s system. First, what people like Moore get right:
How is Cuba healthy while poor? Most attribute the fact to Cuba’s zero monetary cost health care system. There is some truth to that attribution. With 11.1% of GDP dedicated to health care and 0.8% of the population working as physicians, a substantial amount of resources is directed towards reducing infant mortality and increasing longevity. An economy with centralized economic planning by government like that of Cuba can force more resources into an industry than its population might desire in order to achieve improved outcomes in that industry at the expense of other goods and services the population might more highly desire (pg. 755).
However,
Centralized planning has disadvantages. Physicians are given health outcome targets to meet or face penalties. This provides incentives to manipulate data. Take Cuba’s much praised infant mortality rate for example. In most countries, the ratio of the numbers of neonatal deaths and late fetal deaths stay within a certain range of each other as they have many common causes and determinants. One study found that that while the ratio of late fetal deaths to early neonatal deaths in countries with available data stood between 1.04 and 3.03 (Gonzalez, 2015)—a ratio which is representative of Latin American countries as well (Gonzalez and Gilleskie, 2017). Cuba, with a ratio of 6, was a clear outlier. This skewed ratio is evidence that physicians likely reclassified early neonatal deaths as late fetal deaths, thus deflating the infant mortality statistics and propping up life expectancy. Cuban doctors were re-categorizing neonatal deaths as late fetal deaths in order for doctors to meet government targets for infant mortality.
Using the ratios found for other countries, corrections were proposed to the statistics published by the Cuban government: instead of 5.79 per 1000 births, the rate stands between 7.45 and 11.16 per 1000 births. Recalculating life expectancy at birth to account for these corrections (using WHO life tables and assuming that they are accurate depictions of reality), the life expectancy at birth of men by between 0.22 and 0.55 years (Gonzalez, 2015) (pg. 755).
But that’s not the only thing driving low infant mortality rates:
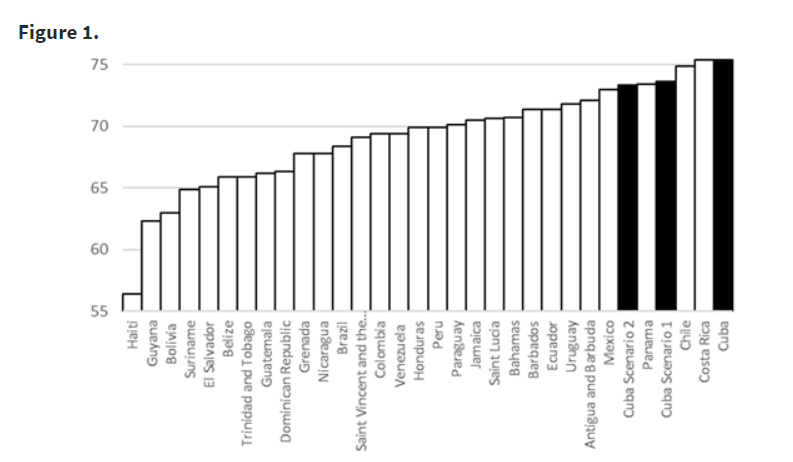
Coercing or pressuring patients into having abortions artificially improve infant mortality by preventing marginally riskier births from occurring help doctors meet their centrally fixed targets. At 72.8 abortions per 100 births, Cuba has one of the highest abortion rates in the world. If only 5% of the abortions are actually pressured abortions meant to keep health statistics up, life expectancy at birth must be lowered by a sizeable amount. If we combine the misreporting of late fetal deaths and pressured abortions, life expectancy would drop by between 1.46 and 1.79 years for men. In Figure 1 below, we show that that with this adjustment alone, instead of being first in the ranking of life expectancy at birth for men in Latin America and the Caribbean, Cuba falls either to the third or fourth place depending on the range (pg. 755-756).
The researchers explain, “Other repressive policies, unrelated to health care, contribute to Cuba’s health outcomes” (pg. 756) These include:
- Restrictions in car ownership leading to low automobile fatalities.
- Rationing combined with physically demanding transportation (e.g., cycling) contributing to reductions in obesity and deaths caused by diabetes, coronary heart diseases and strokes.
The researchers conclude,
Cuban mortality and longevity statistics appear impressive. They are a result of some combination of the government’s choice to allocate more resources into the health care industry (at the expense of other industries that could produce needed goods) and from coercive measures through both health delivery and economic planning that improve health statistics at the expense of other spheres of life.
Although the USA and other countries re-examine how to design health care delivery they should not uncritically accept the myth that the Cuban health care system has been the sole, or even the most important, cause of Cuba’s abnormally high longevity statistics. The role of Cuban economic and political oppression in coercing ‘good’ health outcomes merits further study (pg. 756).
This is my first time pay a visit at here and i am genuinely impressed